Healthcare still runs on the fax machine. In a field that can sequence a genome, a prior authorization often travels by fax, gets re-typed into a portal by hand, and waits. That gap, between clinical sophistication and administrative duct tape, is where robotic process automation in healthcare earns its keep.
The point is not to put AI between a clinician and a patient. The point is to take the swivel-chair work, the copying of the same number from one system into three others, off the people doing it. Healthcare is staffed by expensive, trained, burned-out humans spending a meaningful slice of their week on data entry. Automation gives that time back. The patient never sees it, which is exactly the point.
This guide is the practical version: what RPA and automation in healthcare actually are, how the pieces work, the use cases worth doing first, where the ROI comes from, and the compliance realities you cannot skip in a regulated vertical.
What is RPA in healthcare?
Robotic process automation in healthcare uses software "bots" to carry out high-volume, rules-based tasks the way a person would, but without the person. The bot logs into the systems, reads a field, applies a rule, and types the result into the next system. Eligibility verification, claim status checks, moving data between an EHR and a billing platform. The repetitive, deterministic work that follows a clear set of steps.
It helps to separate three terms that get used interchangeably.
RPA handles the rule-based, repetitive steps. If a human does it the same way every time by following instructions, a bot can do it. No judgment required.
AI handles the judgment. Reading an unstructured referral letter, extracting values from a scanned lab, predicting which claims will deny. AI deals with the messy, the unstructured, and the probabilistic, where RPA needs things clean and predictable.
Healthcare automation is the umbrella over both, plus the integration plumbing that connects systems. In practice a real solution blends them: RPA for the structured steps, AI for the parts a rule cannot read, and integration so they share data. The good projects know which tool is doing which job, and do not pay for a model to do an if-statement.
You will also hear "intelligent automation" and "hyperautomation" for this blend of RPA plus AI plus integration. The label matters less than the discipline behind it. A bot that mimics a human clicking through a screen is the most fragile version, useful where a legacy system offers no other door, and a problem the morning a vendor moves a button. Wherever a system exposes a real interface, integrating through it instead is the version that survives. The goal is automation that bends, not breaks, when the world around it changes, which in healthcare IT it does constantly.
How healthcare automation works
Strip away the branding and the mechanism is straightforward.
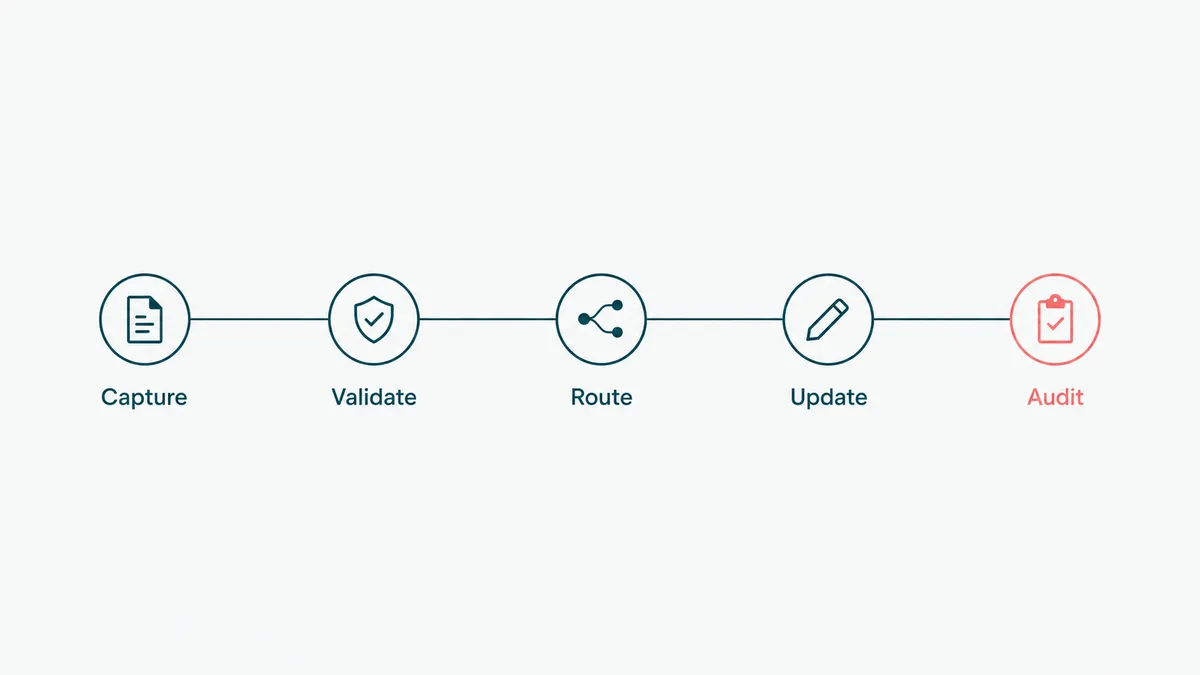
A trigger starts the process: a new claim, a scheduled time, an inbound document, a status change in the EHR. The automation wakes up, gathers the inputs it needs from the relevant systems, applies the rules (and a model where the input is unstructured), takes an action, files a claim, updates a record, sends a notice, and logs what it did. When something does not fit the rules, a missing field, an ambiguous code, a record that does not match, a well-built automation does not guess. It flags the case to a human and moves on to the next one, so the exceptions get judgment and the routine gets speed.
The hard part is the systems. Healthcare IT is a museum of formats that were never meant to talk: an EHR like Epic or Cerner, a separate billing platform, a clearinghouse, a scheduling system, a patient portal, and an alarming amount of fax and PDF. Real automation has to reach into all of them. Where a system exposes a proper interface (an API or an HL7/FHIR feed), we integrate through it, which is durable. Where it does not, RPA can drive the user interface as a last resort, though screen automation breaks the morning someone moves a button, so it is the door of last choice, not first.
This is why integration, not the bot, is the actual project. An automation that cannot read your EHR can only pretend to help. If you want the connective tissue done properly, that is healthcare API integration work, HL7, FHIR, and EHR feeds, and it is usually the part that determines whether the whole thing holds up.
Two more distinctions that shape a real deployment. Unattended bots run on their own on a schedule or a trigger, the back-office automation that works overnight. Attended automation runs beside a person, assisting in real time, which suits anything touching a clinical decision. And a fair amount of healthcare input is still unstructured, faxed referrals, scanned IDs, PDF lab results, so a model that reads documents and turns them into structured data is often the first AI step that earns its place, feeding clean inputs to the rules that follow. Yes, the fax thing is real. We are as surprised as you are.
Healthcare automation use cases
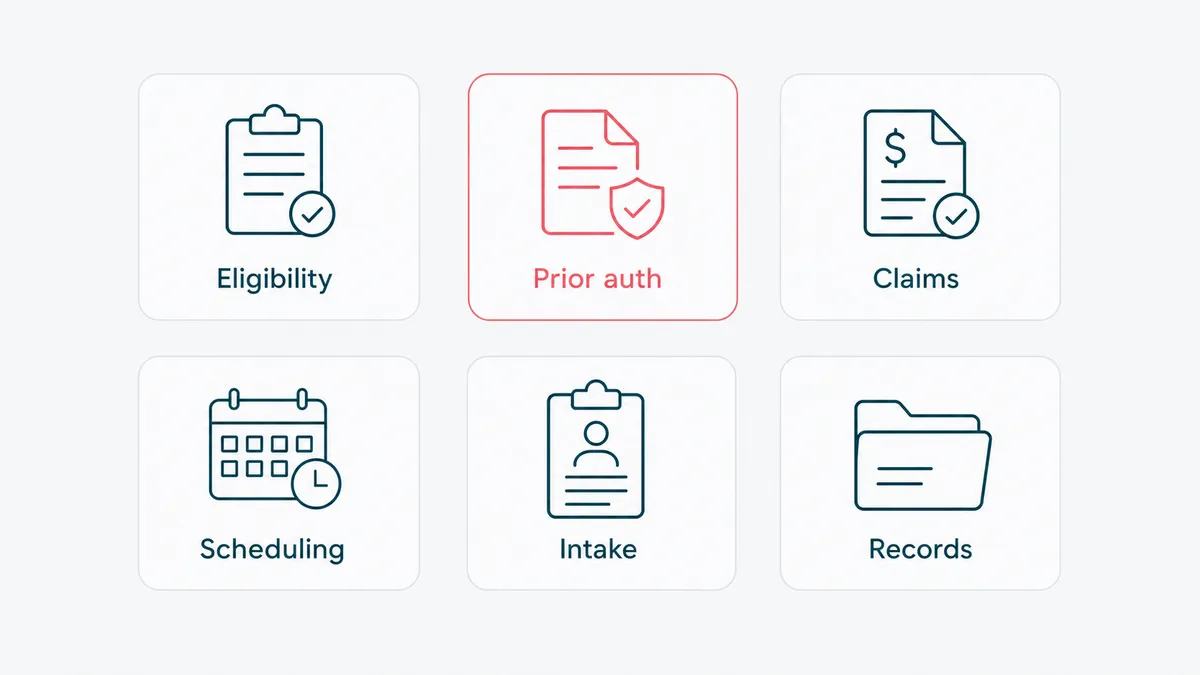
The administrative side is where automation pays back first and most reliably. Here are the use cases worth knowing.
Claims processing and revenue cycle
The big one. Automating claim creation, scrubbing, submission, status checks, and denial triage across the revenue cycle. Claims are high-volume, rule-heavy, and expensive when they go wrong, which is the exact profile automation handles best. Bots check claims against payer rules before submission, catching the errors that cause denials, and chase status so a human is not refreshing a portal all afternoon. The Centers for Medicare and Medicaid Services publishes the program rules these workflows have to follow, and encoding them correctly is most of the value. Denials are the place the money leaks: a claim that denies is rework, delay, and sometimes write-off, so catching the avoidable ones before submission is often the single line item that funds the whole automation program.
Prior authorization
The poster child for healthcare's administrative pain. Prior auth is slow, manual, and universally hated, by patients waiting on care, by clinicians filling out forms, and by the staff chasing payers. Automation gathers the required clinical documentation, submits the request, and tracks the response, cutting the days of back-and-forth that delay treatment. This is also where RPA and AI combine: a model reads the clinical notes to assemble the justification, RPA submits it through the payer's process, and a person reviews anything ambiguous before it goes out. The work that used to eat a nurse's afternoon becomes a queue she only touches for the exceptions.
Eligibility and benefits verification
Checking whether a patient's coverage is active and what it covers, before the visit instead of after the claim denies. Done manually it is a staffer on hold with a payer, one patient at a time. Automated, it runs in the background against payer systems for the whole next-day schedule and flags the problems early, when they are still fixable and before they become a surprise bill. Front-desk staff stop being a call center and go back to being a front desk.
Patient scheduling and registration
Automating appointment booking, reminders, intake form collection, and registration data entry. This reduces no-shows and gets clean data into the system without front-desk staff re-keying it from a clipboard. It also frees the front desk to be human with the person standing in front of them.
Data entry and migration between systems
The quiet workhorse. Moving data between the EHR, billing, lab systems, and registries without a human as the copy-paste bridge. Especially valuable during a system migration, where the alternative is a small army temporarily employed to retype records, with the typo rate that implies. The same plumbing keeps systems in sync day to day, so a demographic change made at the front desk does not have to be re-keyed into three other systems by three other people who each get one digit wrong.
Appointment reminders and patient outreach
Automated reminders, recall notices, and follow-up outreach across text, email, and voice. Fewer no-shows, fewer "where is my result" calls, and proactive nudges for care gaps like an overdue screening. No-shows are pure lost capacity, an empty slot that could have been a patient, so even a modest reduction adds real throughput without adding staff. Outreach has to respect patient consent and contact preferences, so the guardrails matter as much as the message.
Compliance and regulatory reporting
Assembling the data for quality and regulatory reporting automatically instead of by quarterly fire drill. Because every automated step is logged, the audit trail builds itself, which a regulated organization will appreciate the first time it gets asked to prove something. The same logging that makes an automation trustworthy also makes the audit defensible, two birds, one well-kept record.
Benefits and ROI of healthcare automation
Where the return actually comes from, in rough order of reliability.
Lower administrative cost. The work shifts from expensive human hours to software. In a sector where administrative overhead is a notorious share of spend, automating the highest-volume back-office tasks is direct, measurable savings.
Fewer errors and fewer denials. Bots do not get distracted on a Friday afternoon and transpose a number. Catching claim errors before submission means fewer denials, which means faster, more complete reimbursement, often the line item that funds the whole project.
Staff time and burnout. Giving clinicians and admin staff their time back is not a soft benefit in a sector fighting a staffing crisis. Less time on keystrokes is more time on patients, and a job people stay in. Administrative burden is one of the most-cited drivers of clinician burnout, and burnout is expensive twice over, once in turnover and again in the care quality that slips when people are stretched. Automation that removes the busywork is, indirectly, a retention strategy.
Faster throughput. Eligibility cleared before the visit, prior auth that does not take a week, registration that is already done. The patient moves through the system faster, which is both a cost win and a care win.
One honest caution on the ROI math. Automating a broken process just makes you do the wrong thing faster. The biggest returns come from fixing and then automating the high-volume administrative work, not from buying the flashiest clinical AI in the demo. The boring back-office automation pays back first. The clever stuff comes after, once the plumbing is sound.
To know whether it worked, pick the numbers before you start. The honest ones in healthcare automation are concrete: clean-claim rate and denial rate on the revenue-cycle side, hours of staff time returned per week, prior-auth turnaround in days, no-show rate, and the error rate on whatever was being re-keyed by hand. Capture a baseline first, automate one process, and compare. A program that cannot point to a moved number after a quarter is either solving the wrong process or hiding from the measurement, and in a regulated, margin-pressured sector neither is acceptable.
Implementation challenges and HIPAA compliance
This is the section a generic automation vendor skips, and the one that decides whether your project is an asset or an incident.
HIPAA is not optional and not a footnote. Any automation touching protected health information has to satisfy the Privacy and Security Rules: access controls, encryption in transit and at rest, audit logging of every access, and a Business Associate Agreement with any vendor that touches PHI. The US Department of Health and Human Services publishes the HIPAA rules, and "the bot needed the data" is not a defense. Build the controls in from the first line, because retrofitting compliance onto a working automation is more expensive than doing it right, and far more expensive than a breach.
Minimum necessary access. A bot should see exactly the data its task requires and nothing more, with its access scoped and logged like any other user. An automation with a god-mode service account is a single point of catastrophic failure. Scope it down.
Auditability. Every automated action on PHI needs to be logged, attributable, and reviewable. The upside is that a well-built automation produces a cleaner audit trail than the manual process it replaced, because a machine does not forget to write it down.
Vendors and data residency. Every third party an automation touches PHI through is part of your compliance surface, which means a Business Associate Agreement and real diligence on where the data lives and who can see it. This is also where the cloud-AI question gets sharp: sending protected health information to a model is a data-sharing decision, not a technical detail, and it needs the same scrutiny as any other vendor. The honest answer is sometimes to keep the sensitive step on infrastructure you control rather than hand it to whatever API is convenient this quarter.
Legacy systems and integration risk. Healthcare IT is old and brittle in places. Integrating safely without destabilizing a system clinicians depend on requires care, testing, and a rollback plan. This is engineering work, not configuration.
Change management and the human factor. Staff are rightly cautious about automation near patient care. The teams that succeed bring clinicians and admin staff into the design, automate the work people already hate, and prove safety on low-risk processes before going near anything clinical. The teams that impose it from a slide deck get quiet resistance and shadow workarounds.
This is exactly the kind of work most software shops avoid on purpose, which is the reason we built the company around it. If HIPAA-aligned delivery is the bar, that is our HIPAA-compliant software development practice, and it is not a checkbox we add at the end.
Healthcare automation companies: build, buy, or partner
Once you decide to automate, the next question is who does it. There are three honest routes, and the right one depends on how specific your processes are and how much you want to own.
Off-the-shelf RPA platforms and healthcare-specific vendors get you moving fast on standard workflows. If your process is common, eligibility checks, a typical claims flow, and a packaged tool already covers it and meets your compliance needs, use it. The cheapest automation is the one you do not have to build, and any honest partner will tell you when that is the situation.
Custom build is for the work the packages cannot fit: processes that span systems that do not talk, exceptions a template never anticipated, or data you cannot hand to a third party. Here you want rpa services for healthcare from a team that has shipped in a regulated environment, not a generic automation shop learning HIPAA on your project.
Whichever route, the things to check are the same. Does the company actually understand HIPAA, or does it say "HIPAA-compliant" and change the subject. Will it sign a Business Associate Agreement. Has it integrated with real clinical and billing systems, EHRs, clearinghouses, and payer portals, or only with tidy demo data. Does it scope minimum-necessary access and log every action. Healthcare automation companies are not interchangeable, and the difference between a careful one and a cheap one tends to surface at exactly the moment a regulator or an auditor asks a question.
How HighCraft builds healthcare automation
We are a senior team that pairs full-stack engineering with applied AI, and healthcare is where we have done the work most shops avoid. We earned Top Rated and a 100 percent Job Success Score on Upwork one delivery at a time, the founder has eleven years in engineering including a FinTech team at a Big Four firm, and our delivery is HIPAA-aligned by default.
A concrete example, kept anonymized. We built a HIPAA-aligned EMR and patient portal for a healthcare wellness platform, in .NET, Azure, and Stripe. It handled intake, clinical workflows, AI-assisted lab analysis that turns a patient's lab PDF into plain language a provider can use, and a full billing system, all under real regulatory scrutiny, on a normal sprint cadence. That is the same stack of skills healthcare automation needs: integration into clinical and billing systems, AI where the input is unstructured, and the compliance discipline to run it safely.
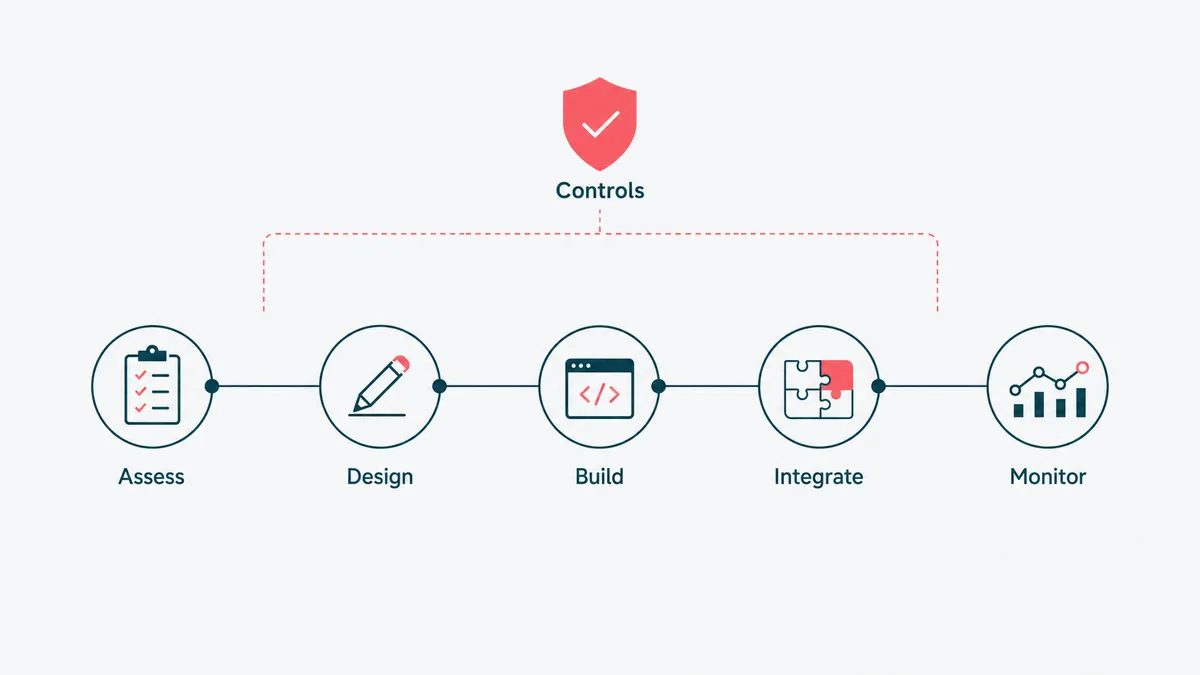
Our shape is consistent. We assess your processes to find where automation pays back without touching clinical risk. We design the workflow and split it honestly into deterministic rules and the judgment steps that need a model. We build the automation and the AI agents where they belong. We integrate over your real interfaces, and where a system has no door we treat screen automation as the last resort, not the default, the same discipline good business process automation uses everywhere. And we wrap it in monitoring, logging, and an escalation path, so it runs safely and proves it.
We de-risk it the same way every time: start with one high-volume, low-clinical-risk process, prove it against a baseline, then widen. Compliance is designed in from the first line, not bolted on before launch, because in healthcare a retrofit is the expensive path and a breach is the catastrophic one. And we are honest about scope. If an off-the-shelf tool already covers a standard workflow and meets your compliance needs, we say so before quoting a build, because the goal is the automation that pays back, not the biggest invoice.
You work with the engineers who build the system, not a sales layer in front of them. If automation in your organization keeps dying on the integration or the compliance, that is the part we are built for.
Send the processes and the systems they touch, and we will tell you honestly what is worth automating, what should wait, and what a packaged tool already handles for less. We will also, in all likelihood, find a fax machine still load-bearing in there somewhere. We make our peace with it so your staff do not have to.