Two healthcare systems walk into an integration. One speaks a language from 1987, the other from 2014, and somehow you are expected to make them get along. Welcome to HL7 versus FHIR, the most consequential acronym fight in healthcare software. (It is no Ali versus Frazier, but the stakes for your data are surprisingly high.)
HL7 and FHIR are both healthcare data standards, but they come from different eras. HL7 v2 is the older messaging format that still moves most clinical data between systems. FHIR is the modern, web-friendly standard built on REST and JSON that everyone is moving toward. Knowing which one you are dealing with decides how hard your integration will be.
We build the integrations that tie healthcare systems together, so this is the topic we argue about at lunch. Here is the version without the spec-committee vocabulary.

What HL7 (v2) actually is
HL7 version 2 has been the workhorse of healthcare data exchange since 1987. When a lab result lands in a hospital system, odds are it traveled as an HL7 v2 message: a terse, pipe-delimited string that looks like someone sat on a keyboard, but that carries a structured clinical event.
It is everywhere, it is battle-tested, and it is genuinely hard to love. The format predates the modern web, the learning curve is steep, and every vendor has its own dialect. But it runs an enormous amount of the infrastructure your shiny new app will need to talk to, so you do not get to ignore it.
What FHIR is, and why everyone moved
FHIR, which the standards people insist you say as "fire," arrived in 2014 and did the radical thing of being pleasant to work with. It is built on REST APIs and JSON, the same web technologies the rest of software already uses, and it was written with implementers, not committees, as the audience.
That is the whole appeal. A developer who has built any modern API can read FHIR and get productive in days, not months. It is friendly to web and mobile, it models data as clean resources, and it is where the regulators now point. Rules from CMS and the Office of the National Coordinator pushed FHIR-based APIs for patient data access, which turned a nice-to-have into a mandate. You can read the official spec at hl7.org/fhir if you want the source of truth.

The differences that actually matter
Skip the side-by-side spec war. For a build decision, these are the contrasts that change your week.
| HL7 v2 | FHIR | |
|---|---|---|
| Arrived | 1987 | 2014 |
| Format | Pipe-delimited messages | REST APIs, JSON |
| Learning curve | Steep | Moderate to easy |
| Web and mobile | Awkward | Native |
| Regulatory direction | Legacy support | Mandated for patient access |
The short read: FHIR is easier and where things are going, HL7 v2 is harder and where things already are. Both facts are true at the same time, which is the whole problem.
Is FHIR replacing HL7?
This is the question I get most, and the honest answer disappoints the people hoping to skip the old one. Not soon, and not cleanly.
FHIR is the future of new development. But HL7 v2 runs too much live, critical infrastructure to retire on anyone's roadmap. Hospitals do not rip out working interfaces because a better standard exists. So for years, the real world is both. A modern product exposes FHIR at the edges while still consuming HL7 v2 feeds from the systems behind it. Anyone who tells you to build all-FHIR today has not had to connect to a real hospital lately.

Which one you actually need
It depends on what you are connecting to, which is the answer to almost every integration question.
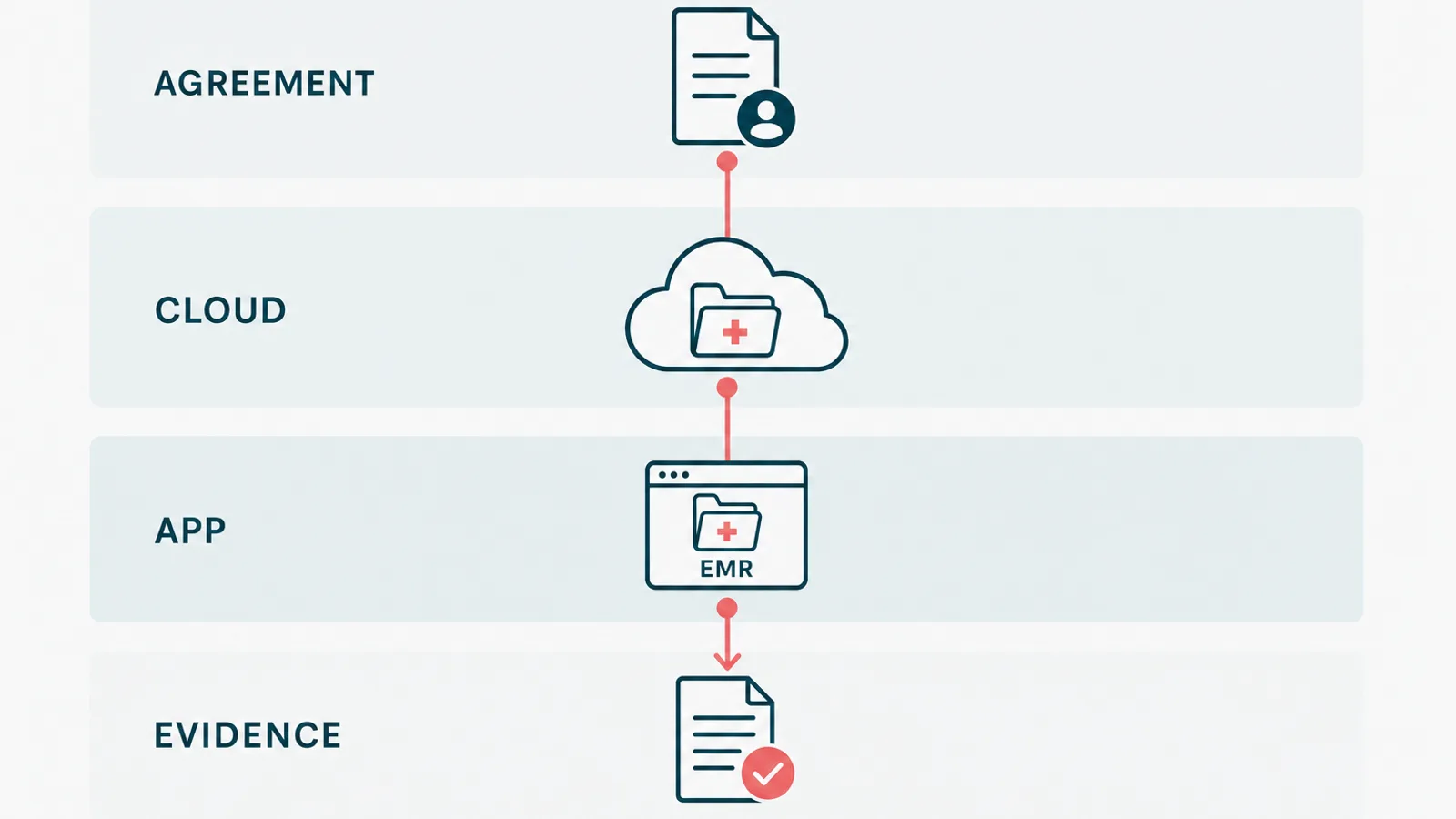
If you are building a new patient-facing app or anything mobile, lead with FHIR. If you have to exchange data with an established hospital, a lab, or an older EHR, you are probably speaking HL7 v2 whether you like it or not. Most builds need a translation layer that does both, so a result arriving as an HL7 v2 message can land cleanly in a FHIR-based app. That translation is the core of real healthcare API integration, and it is where the hours actually go.

Where this bites you in a real build
The standards are not the hard part. The hard part is that healthcare data is messy, vendors interpret the spec loosely, and the edge cases are where patients get hurt if you cut corners.
We built a HIPAA-aligned EMR and patient portal for a healthcare wellness platform. The integrations were the part that earned the budget, not the charting. Patient matching, terminology mapping, and the legacy feeds that refuse to retire are where weeks disappear. If you are scoping an EHR or a custom healthcare platform, assume the interoperability work is bigger than it looks, because it always is. Our guide on how to create EHR software walks through where it fits in the build.
So when someone hands you a clean HL7-versus-FHIR comparison and implies you only need one, smile politely. Then budget for both. If you would rather hand that mess to people who enjoy it, email us. We are the kind of engineers who have opinions about pipe delimiters, and we have made our peace with it.