So you want to build an EHR. Somewhere a hospital CIO just felt a chill and does not know why. (They have seen this movie. It usually has a sequel called The Integration.)
To create EHR software, you start from a clinical workflow, not a database. You build the record and its core charting, then wire in the lab, pharmacy, and billing integrations. HIPAA goes in from the first commit, and you ship a focused version before you attempt the whole thing. The order matters more than the tech stack.
I run a team that builds healthcare software, so take this with the appropriate salt. What follows is the honest version: what you are actually making, the steps that matter, what moves the cost, and the case where you should not build at all.

What you are actually building
An EHR is not a database with a nice front end. It is a clinical workflow, an interoperability layer, and a compliance posture, all running at once. The chart is the easy part. The hard part is that a cardiologist, a pediatrician, and an urgent care clinic all mean different things by the word "visit," and the software has to respect that.
That is why generic EHRs frustrate people. They flatten every specialty into one template and call it a feature. A custom build earns its cost by fitting the way one kind of clinician actually works, which is also why you scope it narrow before you scope it deep.

The honest steps, in order
Skip the part where someone sells you a twelve-phase methodology. The real sequence is shorter.
- Map the workflow first. Sit with the clinicians and chart a real visit, end to end, before anyone opens an editor.
- Settle the architecture and the data model, because changing how the record is structured later is the expensive mistake.
- Build the core charting and the record, then get it in front of real users fast.
- Wire the integrations: labs, pharmacy, billing, and the systems that already hold your data.
- Layer in compliance and security as you go, not as a panic before launch.
- Decide whether you need formal certification, then deploy, train, and keep maintaining it, because software is never finished.
Notice that "write code" is one line in the middle. The work around it is the work.

What drives the cost and the timeline
Industry guides put a full enterprise EHR at $400,000 to $2,000,000, with a first working version in two to four months. Those are real numbers for a real platform, and they scare people for good reason.
The good news is that you almost never need the two-million-dollar version on day one. Cost tracks four things: the number of clinical workflows, the integrations, the compliance and certification scope, and how much of it you insist on building before you ship anything. The MVP is the lever. Build a focused record for one specialty, get clinicians using it, and let real demand decide what comes next. The features you were certain you needed have a way of going quiet once a provider is actually charting in the thing. We covered this math in detail in our telemedicine app development cost guide, and it applies here too.

Build for a specialty, not for "healthcare"
The fastest way to make an EHR nobody likes is to build it for everyone. Specialties are where custom actually pays off, because the workflow gaps are specific and the off-the-shelf products are weakest.
A cardiology record needs ECGs and echo data in the chart, not as attachments. A cardiology EHR and a dermatology EHR are barely the same product under the hood: one lives on device data, the other on images and lesion tracking. Pediatrics needs growth charts and immunization registries. Pain management needs an airtight controlled-substance trail. Pick the one specialty whose pain you understand best, and build that record properly before you generalize.

The part everyone underestimates
Two things blow up EHR timelines, and they are always the same two: compliance and interoperability.
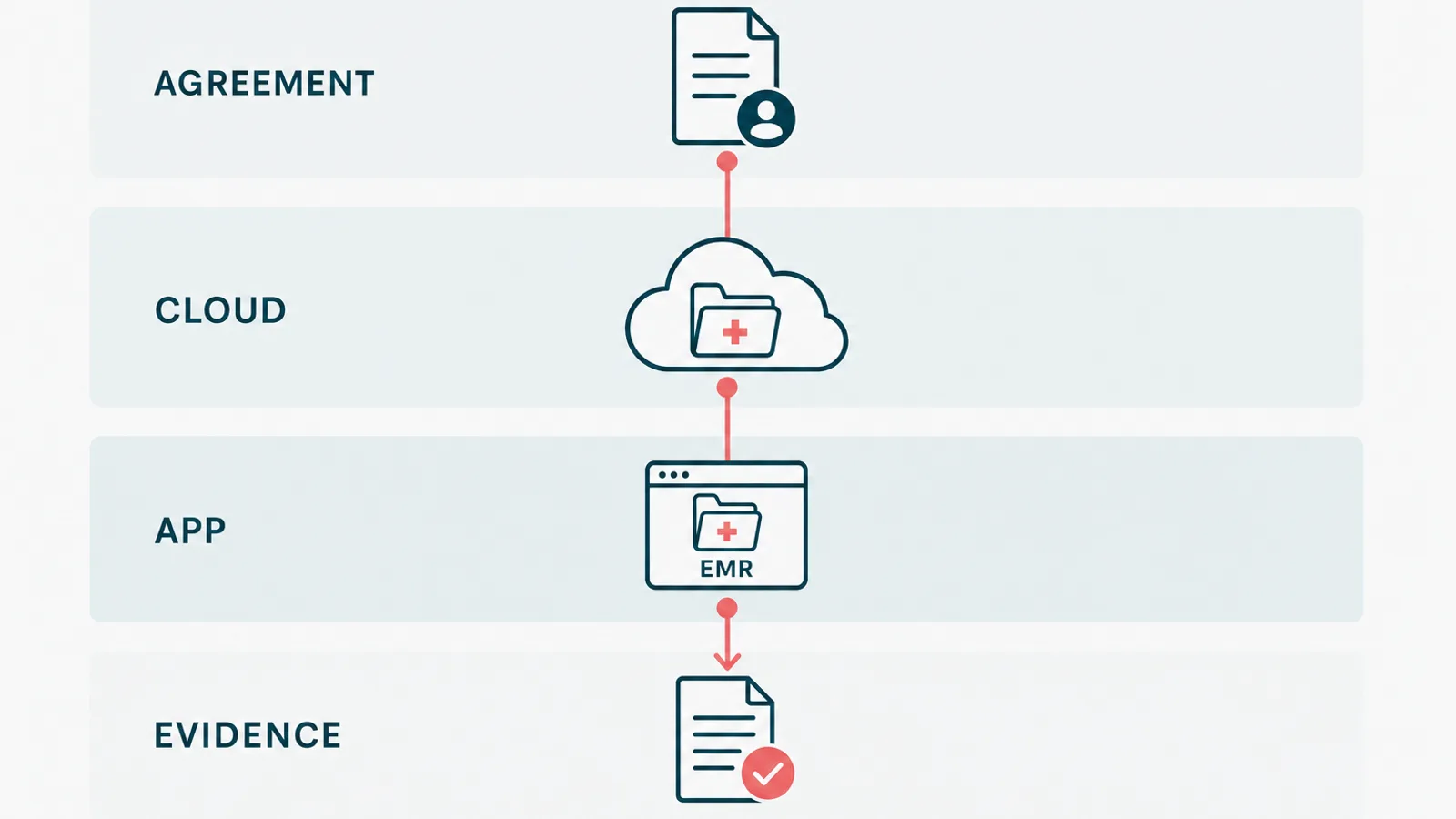
Compliance is not a final checkbox. An EHR handles protected health information, so HIPAA-compliant development has to be in the foundation: access control, audit logging, encryption, and the agreements that follow the data through every vendor. Interoperability is the other one. The moment your record has to exchange data with a lab or another system, you are doing healthcare API integration over HL7 and FHIR, and the hard part is rarely the code. It is the vendor approvals and the data that never matches the spec. The federal interoperability rules at HealthIT.gov are worth reading before you scope, not after.

When you should not build an EHR
Here is the advice the agencies bury, so it goes near the top of the ending. Most practices should not build an EHR.
If a configurable product covers your specialty and you can live inside its workflow, buy it. It is faster, cheaper, and already certified. We turn away EHR builds that an existing product would handle better, because selling someone a two-year project they did not need is the fastest way to lose them for good. We learned where the line sits by building a HIPAA-aligned EMR and patient portal for a healthcare wellness platform, with intake, clinical workflows, AI lab analysis, and billing, under real regulatory scrutiny. The parts that justified custom were the workflow and the integrations, the exact things no off-the-shelf product would bend to. Everything else, we would have told them to buy.
So before you create EHR software, be honest about which side of that line you are on. If you are genuinely past what the standard products can do, custom EHR development is the right call, and we are happy to scope it. If you are not, email us anyway. We will talk you out of it, and we will only make one joke about your legacy HL7 feeds while we do.