Conversational AI in healthcare has been demoed in every hospital boardroom in America by now. Far fewer of those demos ever talk to a real patient. (The gap between the two is, more or less, where I make a living.)
Conversational AI in healthcare is software that holds a real back-and-forth, by text or voice, to finish a clinical or administrative task: intake, scheduling, triage support, patient questions, or follow-up. It runs on language models grounded in the provider's own data, inside HIPAA. Done right, it is a feature a patient actually uses. Done wrong, it is a chatbot nobody opens twice.
Full disclosure: we build this, so I am not a neutral party. But that also means I have shipped the unglamorous parts nobody puts in the demo. This guide covers what conversational AI really does in healthcare, where it works, the HIPAA reality, the gap between a demo and a product, and when a chatbot is the wrong tool entirely.
What conversational AI in healthcare actually means
Start with what it is not. It is not the phone tree that asks you to "press 1 for appointments" and then loses you. It is not a search box wearing a speech bubble. Conversational AI understands what a person means, not just what they typed, and it carries the thread across several turns.
Underneath, it is a language model wired to your systems. The model handles the language. The engineering handles everything that makes the language safe and useful: pulling the right record, staying on topic, and knowing when to hand off to a human. By text, by voice, or both.
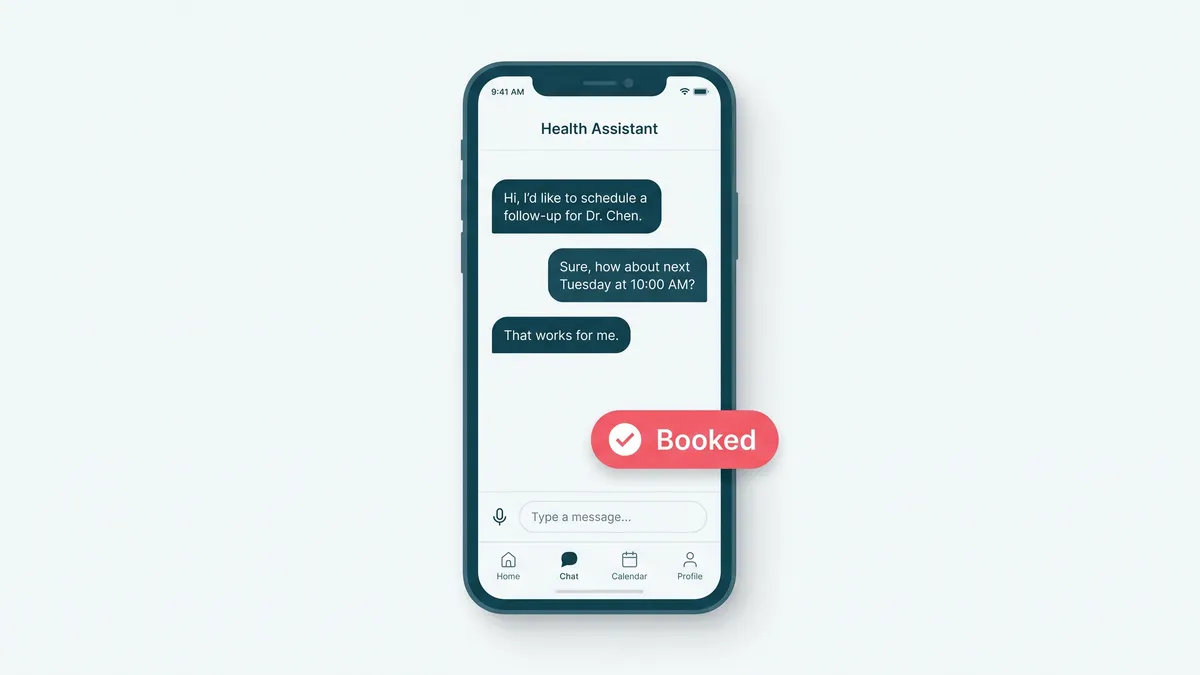
The distinction that matters is task completion. A chatbot answers a question. A conversational AI finishes a job: the appointment is booked, the intake is structured, the prescription refill request reaches the right queue. If it just talks, it is decoration.
Where it works: the use cases that ship
The wins are concentrated in two places: administrative load and patient communication. That is not a knock. Administrative load is where clinicians lose their evenings.
- Patient intake, asked one question at a time, with the answers landing as structured data instead of a wall of free text.
- Appointment scheduling and reminders, including the reschedule nobody wants to make over the phone.
- Symptom navigation that routes a patient to the right level of care. Routing, not diagnosing.
- Billing, prep, and results questions, answered from real policy instead of a guess.
- Post-visit follow-up and adherence check-ins, the ones a busy practice never gets to.
- Ambient documentation that drafts the visit note, so the clinician edits instead of types.
Most of these are conversations a human would do if a human had the time. That is the tell for a good fit. If you want to take this further into a patient-facing build, that is the territory of mental health app development and broader healthcare AI consulting, where the conversation is the product, not a bolt-on.
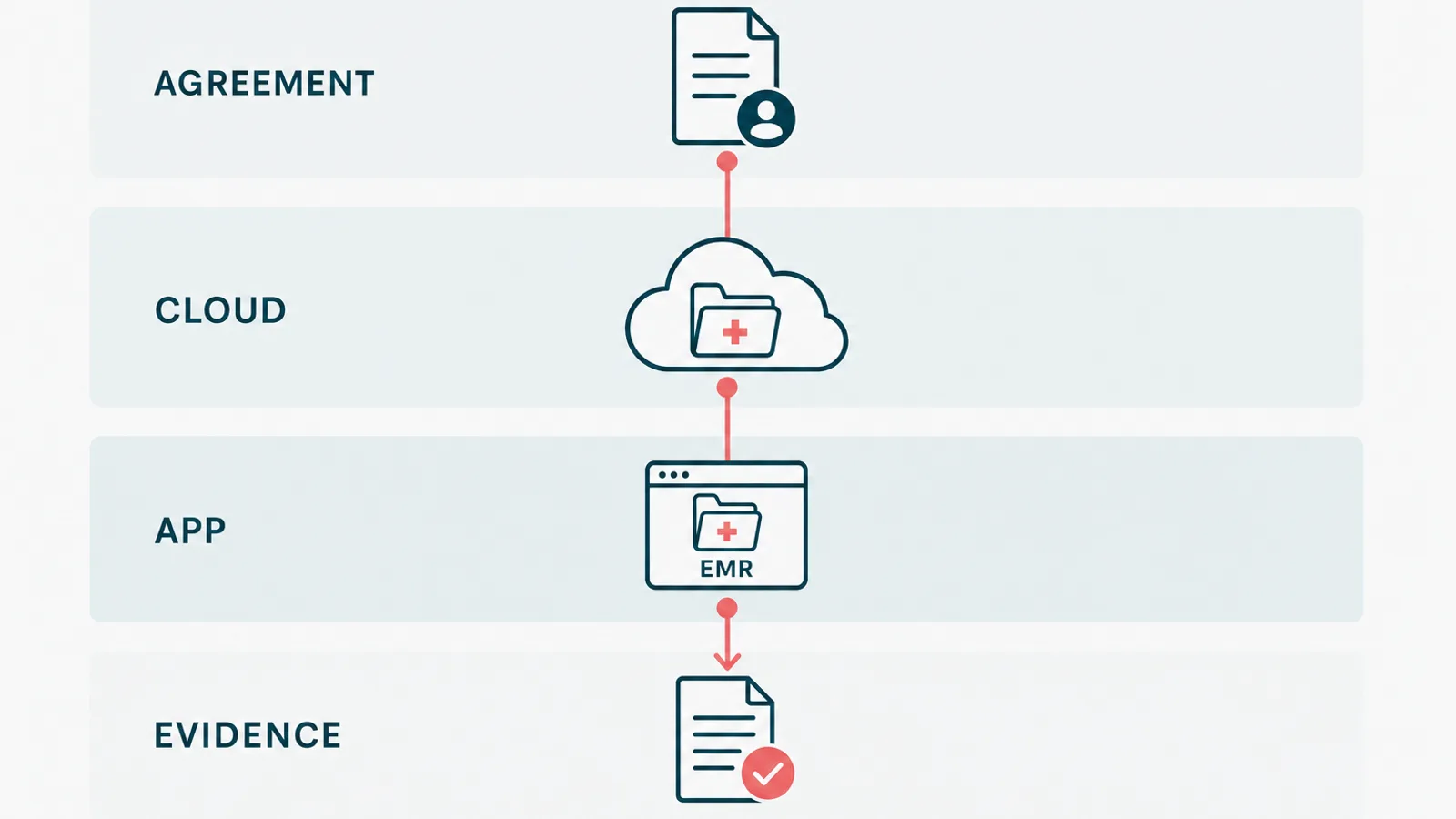
The HIPAA part everyone skips in the demo
Here is the slide that never makes the pitch deck. The moment your assistant touches a name, a date of birth, or a diagnosis, it is handling protected health information, and HIPAA applies.
That changes the engineering, not just the paperwork. You need a signed BAA with whoever runs the model. You need access control and audit logging on every exchange. And you need a model path that does not quietly train on, or leak, your patients' data. A consumer chatbot endpoint does not clear that bar. A governed deployment, like Azure OpenAI under a Microsoft agreement, can.
The boring correctness is the whole job here. We have shipped it before: encryption, audit trails, and consent handled from the first commit, not bolted on the week before a security review. If a vendor's HIPAA answer is "we are working on it," that is your answer too.
The gap between a demo and a product
This is the part I would tattoo on a whiteboard if whiteboards held ink that long. A demo that works most of the time is easy now. A system you put in front of a patient at ninety-nine percent is not, and the distance between them is the actual engineering.
What you show the model matters more than how you phrase the request. Going from zero examples to a handful of good ones, around fifteen, is the cheapest accuracy win there is, and closing the gap from roughly ninety percent to ninety-nine is what turns a demo into something a clinic can trust. That gap is retrieval, evaluation against real cases, and a human in the loop where a wrong answer is expensive. The model is a part, not the product.
This is why "which model do you use" is the wrong first question. The model is a swappable component. The grounding, the eval harness, and the guardrails are the build. We go deeper on that in why context beats the prompt, and it is the spine of how we approach generative AI development generally.
An example a clinician actually opened
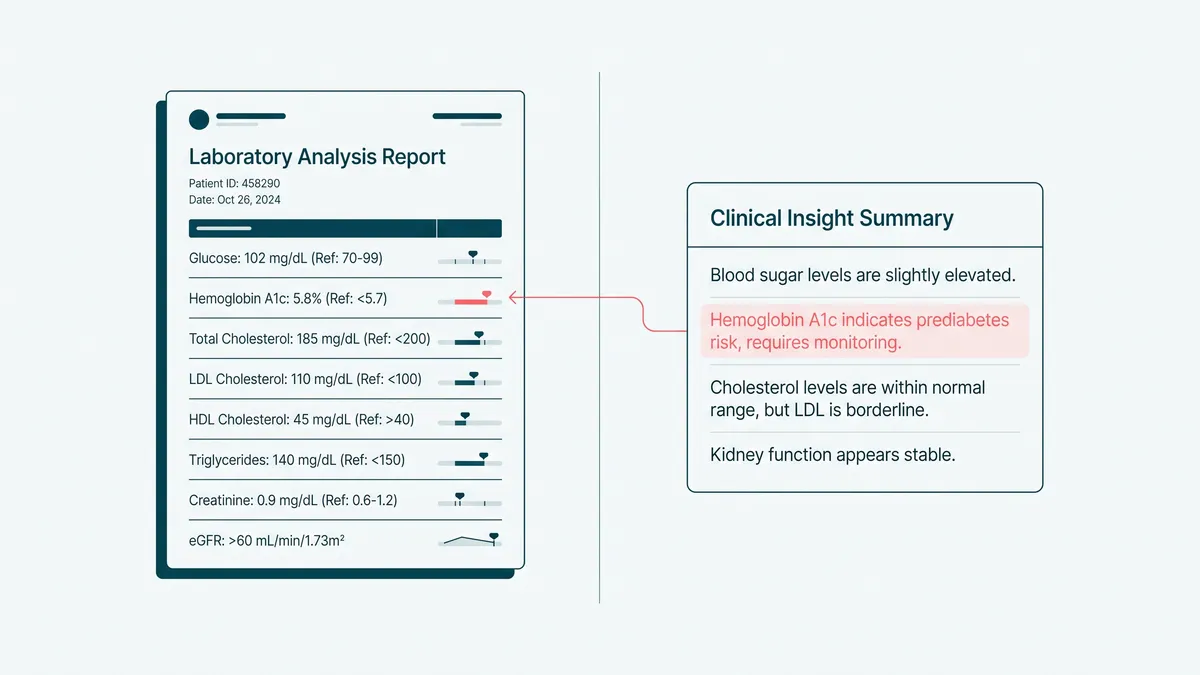
On a HIPAA-aligned platform we built, we shipped AI-assisted intake that reads a patient's lab PDFs. It pulls out the values and turns them into plain language a provider can use during the call, instead of jargon that scares the patient before the visit even starts.
We held it to one test, and only one: would a provider actually reference this mid-conversation, or is it a feature that wins a meeting and then gathers dust. It passed. Providers opened it because it saved them the translation step they were already doing in their heads.
That is the bar. Not "is the AI impressive," but "does a busy clinician open it a second time." Almost everything else is theater. We wrote more about that line in AI that ships versus AI that demos, because it is the single most useful question to ask any healthcare AI vendor.
When a chatbot is the wrong tool
Now the part that costs me work. Sometimes conversational AI is the wrong answer, and the honest move is to say so.
If the task is a fixed, five-field form, build the form. It is faster, cheaper, and it never hallucinates a date. If the patient just needs one number from one system, a button beats a conversation. And if the question is clinical diagnosis, that is not a chatbot job at all. Route to a clinician and stop.
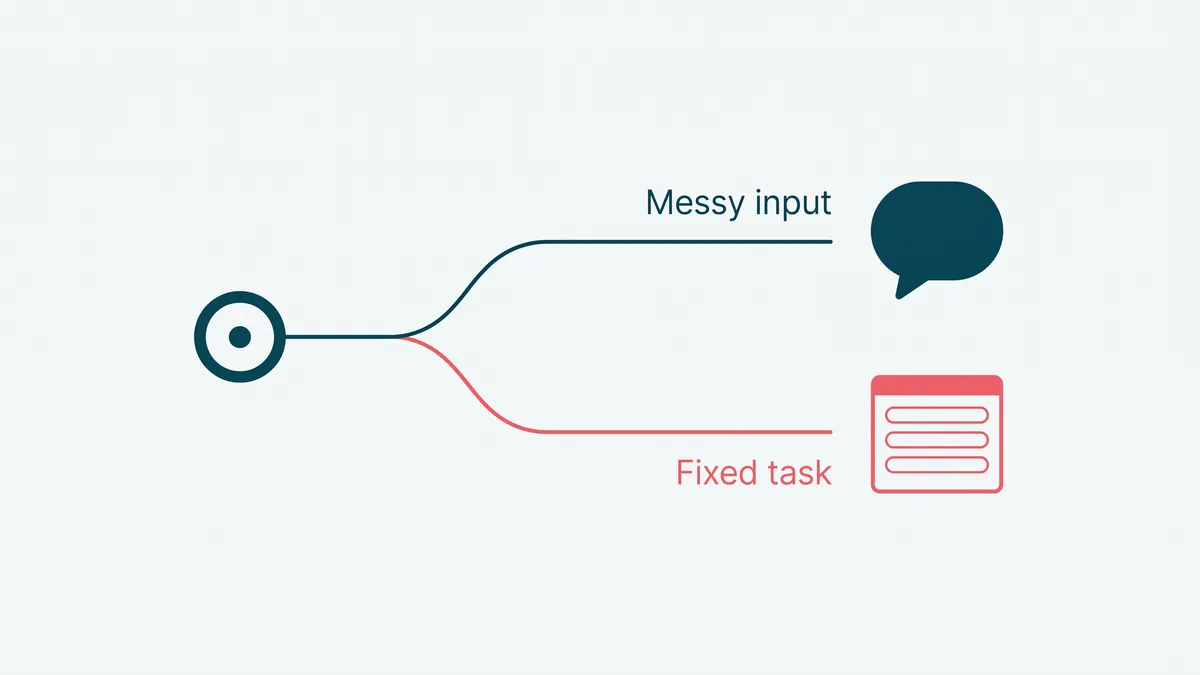
The rule of thumb: reach for conversational AI when the input is messy human language, the path branches, and a person would otherwise spend real time on it. Reach for a plain interface when the task is deterministic. We turn down conversational builds that should have been a well-placed bit of automation more often than you would expect, because a model you do not need is just an expensive way to add a failure mode.
So before you buy the chatbot, ask where it finishes a job a human is doing today. If the answer is specific, you have a project. If the answer is "engagement," you have a demo with a lanyard. We will happily tell you which one you are holding, and if you want a second opinion, email us.